Skin cancer is one of the most prevalent cancers affecting men and women in New Jersey; 1 in 6 of us will develop some form of skin cancer in our lifetime. If you’ve been diagnosed with skin cancer or have a pre-cancerous lesion, we invite you to contact Dr. Parker for a consultation in Paramus, NJ, to discuss your options for tumor removal, and if needed, reconstructive surgery after treatment.
Dr. Parker provides skin cancer treatment for people from Ridgewood, Hackensack, Mahwah, Somerset, and other Bergen County and North New Jersey cities.
Our Experienced surgeon
Dr. Paul M. Parker
Board-certified plastic surgeon Dr. Paul M. Parker combines an unwavering dedication to patient satisfaction with surgical expertise to create aesthetically pleasing, natural-looking results.
What Types of Skin Cancer Surgery Does Dr. Parker Perform?
Dr. Parker is board certified in plastic surgery and has over 25 years of surgical experience. He will work closely with your dermatologist to determine the best course of treatment. He can remove many types of precancerous and cancerous lesions himself. When more extensive cancer surgery is performed by another specialist, Dr. Parker will often perform the reconstructive procedure to help restore a natural appearance to the treated area.
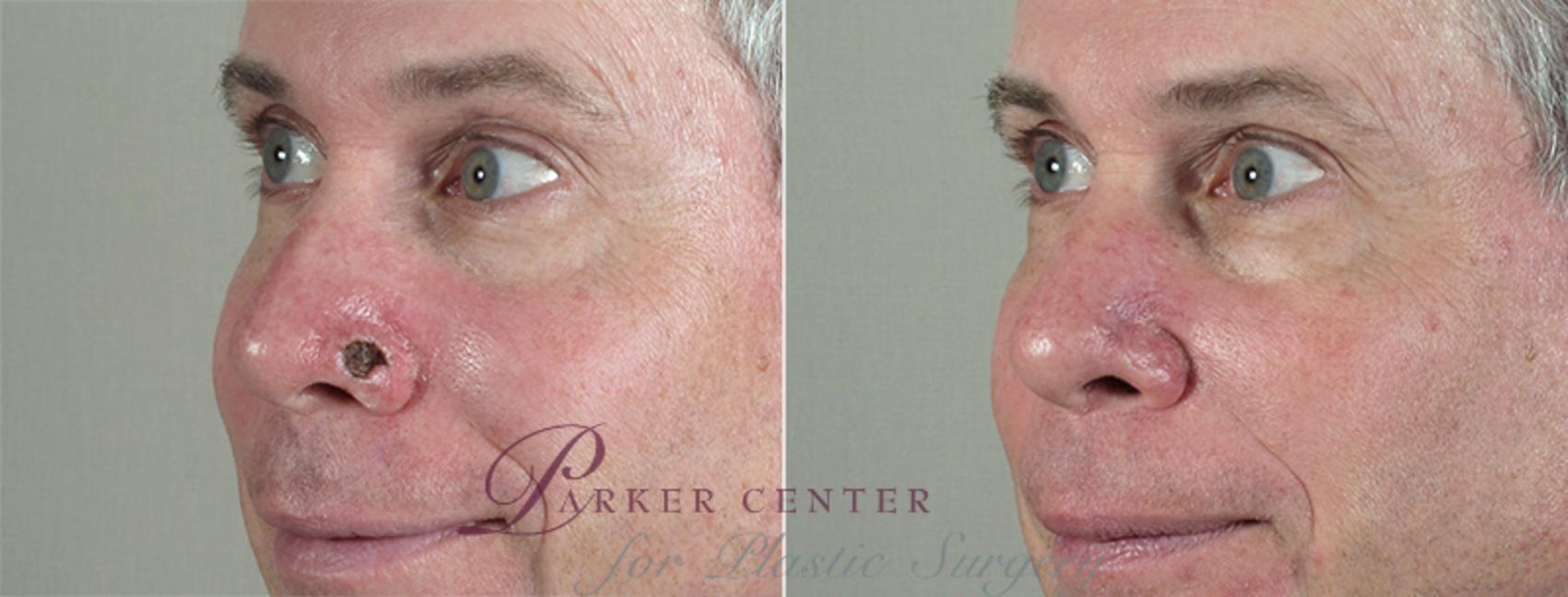
Before & After Skin Cancer Treatment
This patient underwent Mohs surgery to remove a basal cell skin cancer from the left side of his nose. Dr. Parker then reconstructed the defect by shifting adjacent skin and underlying tissues into it to leave imperceptible scarring.
Removing Benign Lesions
If the lesion clearly appears to be benign, based on this evaluation, observation is usually recommended. If the patient and/or family are bothered by the appearance of the lesion, Dr. Parker provides a detailed discussion about removal options. Consideration may be given to shave removal by a dermatologist, and if elected, an appropriate referral is made.
Surgical excision by Dr. Parker and careful soft tissue repair are discussed as well. An anatomic diagram is drawn for the patient, demonstrating how the lesion is to be removed completely. In addition, diagrams are used to demonstrate the use of cosmetic surgical techniques employed by Dr. Parker in his cosmetic surgeries to try to make the resultant scarring as inconspicuous as possible.
Removing Precancerous Lesions
Lesions suspicious for being pre-cancerous or cancerous are treated with a full-thickness skin biopsy, either incisional or excisional, as discussed by Dr. Parker with the patient.
Precancerous lesions are referred to a dermatologist if topical treatment is appropriate. If not, surgical excision by Dr. Parker and careful soft tissue repair are discussed. An anatomic diagram is drawn for the patient demonstrating a more aggressive surgical removal than for benign lesions. In addition, diagrams are used to demonstrate the use of cosmetic surgical techniques employed by Dr. Parker in his cosmetic surgeries to try to make the resultant scarring as inconspicuous as possible.
All of these lesions are reviewed by a pathologist to verify the histology of the lesion and for the completeness of removal.
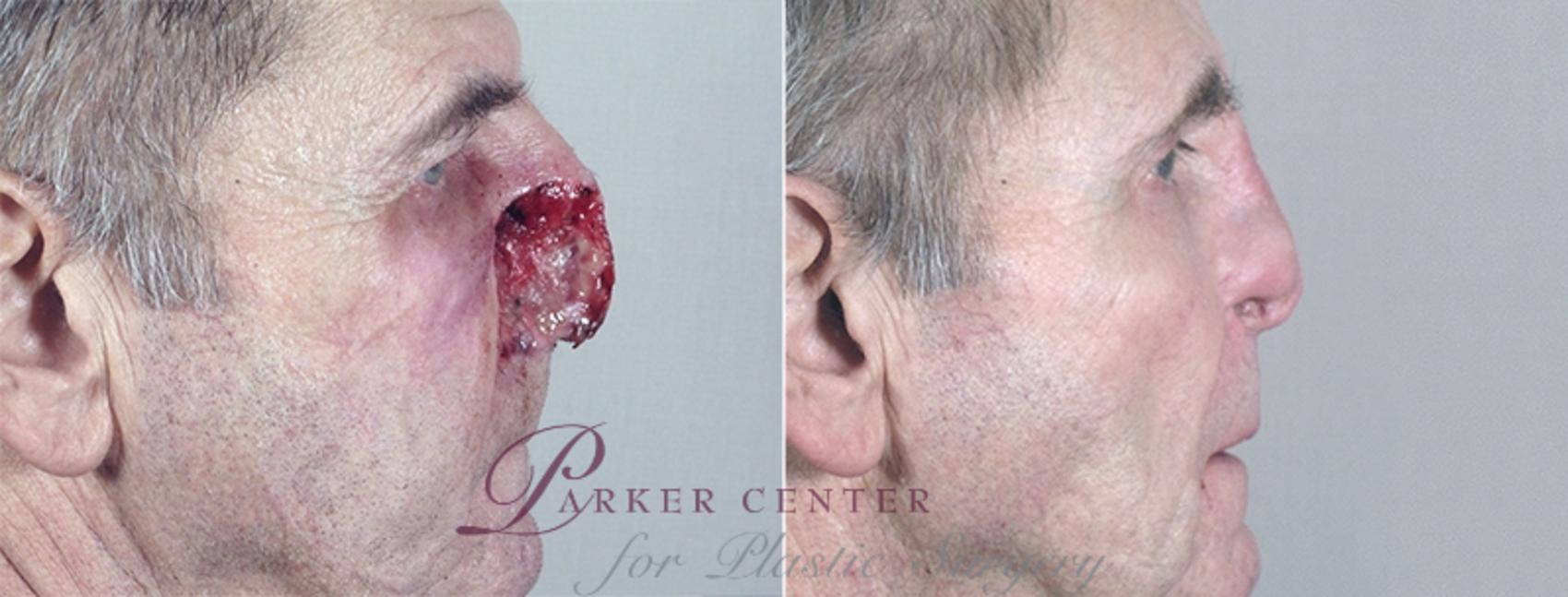
Skin Cancer Treatment Before & After Photos
WARNING:
This feature contains nudity. Please click OK to confirm you are at least 18 years of age and are not offended by such material.
The patient was referred to Dr. Parker for post Moh’s reconstruction of a defect at the base of her nose and upper lip. She had undergone 12 prior skin cancer procedures limiting Dr. Parker’s options for treatment. He discussed with the patient, then performed, a reconstruction of the defect with a full thickness skin graft removed from in fr... Read More
This 68 year old was referred to Dr. Parker for reconstruction of a Mohs defect on the left side of the nasal tip following removal of a large basal cell carcinoma. Dr. Parker reconstructed this rather large defect, in two stages, with a skin flap from the forehead. Read More
This 75 year old was referred by her Mohs surgeon for reconstruction of the defect on her upper nose following removal of a recurrent basal cell skin cancer. Dr. Parker reconstructed this defect with a skin graft, taken from in front of the ear, because of its size and location on the upper nose. Read More
The patient was referred to Dr. Parker for reconstruction of his nose following Mohs surgery to remove a recurrent basal cell skin cancer. Dr. Parker repaired the nasal defect with adjacent skin and fat from his nose, known as a bilobed flap, along with a cartilage graft. Read More
This 60 year old was referred to Dr. Parker for post Mohs reconstruction following the removal of a large basal cell skin cancer involving the skin of the lower forehead and nose as well as the underlying bones. Dr. Parker reconstructed the defect with a forehead flap. Read More
This 69 year old was referred to Dr. Parker by a Moh’s surgeon for reconstruction of a significant defect involving his nose and cheek after removal of an extensive skin cancer by the Moh’s surgeon. Dr. Parker performed an involved reconstruction which included cartilage grafts and soft tissue to the nose and cheek. The patient required 5 ope... Read More
This 72 year old patient was referred to Dr. Parker by the Mohs surgeon who removed the skin cancer from her upper lip leaving her with an extensive defect. Dr. Parker repaired the defect with a flap of nearby skin and subcutaneous tissue from the cheek. The patient is very happy with her results. Read More
This 83 year old was referred to Dr. Parker for post Mohs reconstruction following the removal of a large basal cell skin cancer involving the nasal skin, cartilage and nasal lining. Dr. Parker reconstructed the defect with cartilage grafts, lining flaps and a forehead flap. Read More
Lesions suspicious for being cancerous are treated with a full-thickness skin biopsy, either incisional or excisional, as discussed by Dr. Parker with the patient. Once the diagnosis is known, options for treatment are discussed with the patient.
Mohs Surgery
Mohs micrographic surgery is a specific surgical technique used to treat skin cancer. Typically performed by an experienced dermatologist, the procedure involves progressively removing cancer cell-containing skin layers until only healthy tissue remains. For patients undergoing Mohs surgery with a dermatologist, Dr. Parker offers post-surgical reconstruction.
Learn more about Mohs surgery below.
Surgical Excision With Frozen Section Margin Control (Non-Melanomas)
Patients who do not need Mohs surgery for their basal or squamous cell skin cancers are treated entirely by Dr. Parker. He surgically excises the skin cancer with an appropriate margin of skin. With the patient still on the operating table, a pathologist microscopically evaluates the removed tissue to be sure all peripheral and deep margins are free of tumor. In the great majority of patients, the margins are negative for residual tumor. Occasionally, the pathologist asks Dr. Parker to remove more tissue from a certain area. Once the tumor has been completely excised, the soft tissue defect is repaired.
The resultant size and extent of the soft tissue defect determine the type of reconstruction to be done. Some defects are best repaired with a skin graft (skin removed and transferred from a distant area); others are better suited for a skin flap (the sliding of adjacent skin into the defect). In either case, Dr. Parker utilizes techniques borrowed from his cosmetic surgeries to make the resultant scarring as inconspicuous as possible.
Surgical Excision of Malignant Melanomas
Based on the Breslow thickness (in mm) of the biopsied melanoma, the appropriate surgical excision will be performed. The following peripheral surgical margins are obtained:
In situ: 0.5 cm margin
Less than 1 mm: 1 cm margin
1 to 4 mm: 2 cm margin
Greater than 4 mm: 2 to3 cm margin
The depth of excision extends completely through the skin and subcutaneous layer to the underlying fascia. For tumors greater than 1 mm thick with non-palpable lymph nodes, sentinel lymph node biopsies are discussed.
The resultant size and extent of the soft tissue defect determine the type of reconstruction to be done. Some defects are best repaired with a skin graft (skin removed and transferred from a distant area); others are better suited for a skin flap (the sliding of adjacent skin into the defect). In either case, Dr. Parker utilizes techniques borrowed from his cosmetic surgeries to make the resultant scarring as inconspicuous as possible.
Our Signature
Rapid Recovery Program
Our surgical procedures, anesthesia, medications, and aftercare are tailored to minimize post-operative discomfort and accelerate recuperation.
Mohs micrographic surgery is performed by a specially trained dermatologist using local anesthesia. The treatment involves the progressive excision of the cancer using serial frozen section analysis and precise mapping of the excised tissue until no evidence of remaining tumor exists. Mohs surgery is recommended by Dr. Parker in the following circumstances:
Difficult and high-risk basal and squamous cell carcinomas, including tumors greater than 2 cm in diameter
Tumors located in areas where deep invasion is more likely
Rapidly growing, recurrent, or ill-defined tumors
Tumors located in an area of previous radiation or where perineural invasion is likely
Coordinated reconstruction of the patient undergoing Mohs surgery is performed by Dr. Parker later that same day or the following day. The resultant size and extent of the soft tissue defect determine the type of reconstruction to be done. Some defects are best repaired with a skin graft (skin removed and transferred from a distant area); others are better suited for a skin flap (the sliding of adjacent skin into the defect). In either case, Dr. Parker utilizes techniques borrowed from his cosmetic surgeries to make the resultant scarring as inconspicuous as possible.
Do I Need Mohs Surgery?
Mohs surgery is a highly successful treatment option for the right candidates. Consulting with an experienced dermatologist or board-certified plastic surgeon can help you determine if Mohs is an appropriate procedure for you.
Mohs surgery is used to remove a variety of malignant lesions, with the two most common being squamous and basal cell carcinomas. Depending on the type of lesion, where it’s located, and your doctor’s recommendation, Mohs or surgical excision with frozen section margin control may be suggested for treating skin cancer.
Mohs can treat the following types of malignant lesions:
Squamous cell carcinoma
Basal cell carcinoma
Melanoma
If you are unsure whether you have a malignant lesion or suspect you may have skin cancer, contact your physician immediately.
Will Mohs Leave a Large Scar?
The goal of Mohs micrographic surgery is to preserve as much healthy skin as possible and ensure all cancerous tissue is removed, all while retaining options for reconstructive surgery. Because Mohs surgery is progressive, the extent of tissue removal—and resultant scarring—cannot be fully anticipated. Coordinated reconstruction by a board-certified plastic surgeon is recommended for patients undergoing Mohs surgery with a dermatologist.
Dr. Parker often receives referrals for post-Mohs reconstruction. Coordinated reconstructive surgery is performed by Dr. Parker either soon after the Mohs surgery or on the following day. The extent and type of reconstruction to be done are determined by the resulting size and degree of soft tissue defect after the Mohs procedure.
The potential for visible scarring is present with all surgical procedures, as many factors contribute to the appearance of surgical scars, including the size and location of the defect and unique skin characteristics. Modified Mohs surgery spares more tissue than traditional skin cancer surgery for less noticeable scarring.
Dr. Parker’s extensive experience with cosmetic techniques helps him to make any resulting scars as inconspicuous as possible. Using skin grafting or skin flap techniques, Dr. Parker incorporates suture lines into natural folds and skin lines wherever possible.
Post-surgical scarring improves with time as the surgical site heals, sometimes taking up to a year to fully “settle.” It is important to follow instructions and be patient during the healing process. Stay in communication with your doctors if you have any concerns.
Financing Surgery Makes Dreams Come True
We believe plastic surgery should be accessible to as many people as possible. That’s why we offer financing through lenders that specialize in setting up payment plans for elective cosmetic surgery. We can discuss financing during your consultation.
If, after reviewing options for treatment, Dr. Parker recommends surgery, arrangements will be made by our staff to schedule the procedure in a timely manner.
Dr. Parker performs all surgeries in Surgiplex, LLC, our on-site, fully certified ambulatory surgical facility. Patient safety is of the utmost importance to Dr. Parker and our staff. Many procedures can be performed under local anesthesia. Our team of board-certified anesthesiologists is available to provide general anesthesia or conscious sedation if requested by Dr. Parker and/or the patient.
Our surgical coordinator will obtain pre-certification of the proposed surgical procedure with your insurance carrier prior to your date of surgery. She will communicate the details of the process to you ahead of time in order to make sure everything goes smoothly.
Dr. Parker will communicate with your referring doctor and/or dermatologist by a customized “referral letter,” with a telephone call if necessary. He will also be sure that they receive a copy of your pathology report for your files in the office.
Following surgery, our highly trained nursing staff will review written postoperative instructions with you in detail. They will call you the next day to check on you and answer any questions you might have.
Our goal at Parker Center for Plastic Surgery is to deliver the highest level of service to you before and after your procedure.
My experience was amazing. I had a large cyst removed and was concerned about scarring. Dr. Parker’s work left a barely noticeable line due to the fact that he took the extra time before surgery to check my neck from all angles with me sitting as well as laying down so he could be sure his work would blend in. I did not have any discomfort at all. Dr. Parker and his staff are truly caring and go the extra mile to make sure patients are comfortable and clear about follow-up care. My internist was also impressed during a routine visit shortly after Dr. Parker performed the procedure.”
-Skin Cancer Patient
Patient Education About Skin Cancer
Dr. Parker is passionate about educating patients about skin cancer and has written several articles on the topic, including ways to protect your skin and recognize tumors and detailed information about skin cancer treatment options. We encourage you to read through the following to help educate yourself about what you can do to keep your skin healthy and protected:
We believe plastic surgery should be accessible to as many people as possible. That's why we offer financing through lenders that specialize in setting up payment plans for elective cosmetic surgery. We can discuss financing during your consultation.
1
Results: Dr. Parker is known for remarkable results that may surpass your expectations